#56 – What’s in a name?
Episode Host: Linda Snell

This episode contributes to the understanding of medical education organizational structures. The hosts are discussing different ways of looking at it, and is it all in the name? Or perhaps on what they do?
Episode article
Kerns, S. C., Beck Dallaghan, G. L., Borges, N. J., & Huggett, K. N. (2023). Where Do We Go From Here? An Inventory of Publicly Available Data About Educator Academies, Medical Education Departments, and Offices of Medical Education. Academic Medicine, 10.1097/ACM.0000000000005762.
Episode notes
Background
The ‘why’ of this paper: recent growth of MedEd units of all kinds, and interest in their relationship with other structures within medical schools
Medical education is a complex endeavour – teaching and learning, across the continuum, research, support of the clinical environment for teaching and learning, teachers and learners, fundraising, assessment, QI of education, faculty development, education scholarship…not fun to be a dean these days! Many organizational structures exist to carry out these functions – and for the latter two, in the US, administrative models include offices of medical education, academies of educators, or departments of medical education, centers of MedEd, amongst others.
Which is best suited for what function and context? It is important to know as it affects everything from faculty recruitment, retention, promotions, staffing and budget models, accreditation compliance, not to mention the quality of teaching and education scholarship. CEs may be more interested in some of these than others, but many CEs work in a context with one of these models – which may or may not align with their personal goals.
Prior work had described models and functions internationally, including roles, structures and expectations of medical education departments and offices, faculty perspectives (and as described in a previous podcast about education leaders’ views). The number and roles of these entities are growing and changing, with education scholarship, usually done in departments of MedEd, becoming more emphasized.
Authors’ hypothesis: departments of medical education would be the least prevalent structures identified in U.S. medical schools.
Purpose
“…to inventory the current structures of medical education departments, offices, and academies at U.S. medical schools to explore reporting structure, functions, and characteristics of these entities.”
Methods
This ‘inventory’ was a document review with a primary source – ‘A Snapshot of Medical Student Education in the United States and Canada: Reports From 145 Schools’ (2020), followed by a search of US med school websites, using appropriate key words, then, if necessary, an in depth ‘browsing’ of websites and more extensive web search.
Used a spreadsheet to report type of unit, reporting structure and description. Summarized frequencies of variables. No clear explanation of how varying data interpreted.
We have talked about document reviews before, but I got interested in how we assure ‘rigor’ in this methodology. There’s not much out there specifically about this methodology but if we adopt from something similar (narrative reviews) most relevant steps here are rationale, scope & boundaries, reflexivity to explain interpretation and details on analysis and interpretation. How did these authors do?
Results/Findings
134/171 schools in US and Canada had data.
There were 3 main ‘types’ of units:
| Office of medical education (OME) | Department of medical education (DOM) | Academy of educators (AOE) |
| supports curriculum, student affairs; led by a vice dean or senior associate dean. | supports education scholarship; led by a Chair. | supports faculty development, ‘academic home’; led by a director (+/- board). |
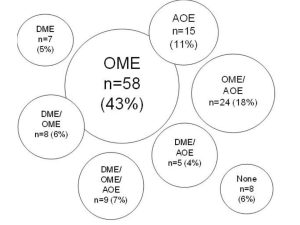
Frequency of types: Some schools had units with dual functions in one office or had >1 entity.
Conclusions
The authors conclude “the least prevalent structure identified was departments of medical education condition … significant because it underscores the difficulty medical education leaders have in obtaining information to research, compare, select, and design the model(s) best suited to support faculty educators at their institution”.
Paper clips
This is limited to US units – and primarily UGME/med school. Other countries have different models and responsibilities, reporting (e.g. to departments), and some standard-setting organizations have individuals or groups who perform similar functions.
‘Previous presentations’ are mentioned – something not (yet) common in our publications – should we be doing this?

0 comments