#33 – Holiday specials
Welcome to the PAPERs podcast Holiday special, where we share some of the most quirky, funny, and surprising papers we’ve come across in our literature search. These are the papers that made us laugh, cry, or scratch our heads in disbelief. These are the papers that we couldn’t resist talking about, even if they’re not the most rigorous or relevant to our practice. These are the papers that will make you say “Wow, I can’t believe this got into the literature!”
So, sit back, relax, and enjoy the show. And if you’re new to the podcast, don’t worry, this is not our usual format. We usually have more serious and thoughtful discussions about the papers we review. But once a year, we like to have some fun and celebrate the diversity and creativity of our field. And who knows, maybe you’ll learn something new or get inspired by some of these quirky papers. So, without further ado, let’s turn to our elves and see what do they have for us!
Fast Forward to Learning: The Effect of Accelerated Playback on Medical Students’ Memory Retention
Elf Jason’s first pick
This paper is for all the people who can’t sit still for too long. It’s about whether it’s okay to watch your medical lectures at double speed.
After the pandemic, we all had to adjust to online videos, and maybe med students have a lot of videos to watch. So, is it okay to watch them at double speed?
Kıyak, Y. S., Budakoğlu, I. İ., Masters, K., & Coşkun, Ö. (2023). The effect of watching lecture videos at 2× speed on memory retention performance of medical students: An experimental study. Medical Teacher, 45(8), 913–917. https://doi.org/10.1080/0142159X.2023.2189537
The authors of this paper did some research and found that it’s actually okay! They even cite previous literature that shows that maybe there’s a threshold. At 1.5 times, your retention is less, so they went through a lot of trouble to conduct a randomized controlled trial. They recruited some medical students and made them watch a video about terminology related to cancer and pathology. They randomized them to one times versus 2 times speed, and they even made them wear a camera so they couldn’t cheat and skip ahead or pause. They did an immediate test and a post-test a week later, and the results were consistent with the accelerated playback hypothesis. The test they gave was just a few MCQ’s, so there are lots of limitations to this methodology. But the bottom line is that for all of us who are a little bit short attention span, it’s okay to watch your neoplasm videos at two times speeds so. This paper is a quick read for you. ??
Does walking help to generate differential diagnosis or are we all too smart for that anyway?
Linda’s article
The paper argues that differential diagnosis is a crucial skill for emergency doctors, and that one common mistake is to stop searching too soon, resulting in a narrow and unoriginal list of possible diagnoses. The paper draws on research from other fields that suggests that physical activity can enhance cognitive performance, and tests whether this applies to medical reasoning as well.
Kaminska, M. E., & Rikers, R. M. J. P. (2022). Does Walking Help to Generate a Differential Diagnosis?. Teaching and learning in medicine, 34(2), 178–186. https://doi-org.proxy.kib.ki.se/10.1080/10401334.2021.1949995
The authors hypothesized that walking while generating a differential diagnosis would lead to more and better ideas than sitting. They conducted a very elaborate experiment to test this hypothesis, but found no significant difference between the walking and sitting groups. They speculated that this might be because the participants, who were senior medical students, had already reached a high level of expertise, and that walking might only benefit novices. They concluded that walking did not impair the diagnostic process, and that it might be beneficial for students’ health and well-being to walk while learning.
What are your thoughts on this? Do you really think medical students walk that slow?
Can can you ever use the word quiet in a clinical department?
Elf Lara’s paper:
We all know the rule: never say “quiet” in a hospital, especially in the emergency department. It’s like inviting chaos and disaster. But is this really true? Or is it just a myth?
That’s what I wanted to find out when I came across this paper by Umar and Jane from Indonesia and Latvia. They published it in the Annals of Medicine and Surgery in 2022. The title caught my eye: “Debunking the myth of using quiet in clinical departments: an integrative overview of available literature”.
Umar, T. P., & Jain, N. (2022). Debunking the myth of using “quiet” in clinical departments: An integrative overview of available literature. Annals of Medicine & Surgery, 82. https://doi.org/10.1016/j.amsu.2022.104792
They searched for studies that tested the effect of saying “quiet” on patient volumes and overcrowding in clinical settings. They only included randomized controlled trials from 2015 to 2022 that were open access. They found five studies that met their criteria.
And guess what? They found no evidence that saying “quiet” made things worse. In fact, most studies (4 out of 5) showed no association between saying “quiet” and patient volumes or overcrowding. So there you have it: it’s a myth. You can say “quiet” without fear of jinxing yourself or your colleagues.
But before you celebrate, you should know that the paper is not very convincing. The authors spend the rest of the paper pointing out the flaws and limitations of the studies they reviewed. They admit that the studies were poorly designed, had small sample sizes, used different definitions of “quiet” and “overcrowding”, and did not account for other factors that could influence patient volumes. They also acknowledge that their own review was not systematic or comprehensive, and that they may have missed some relevant studies.
So, is this paper a diamond or a lump of coal? I would say it’s somewhere in between, but more research is needed so I don’t know John this I’m throwing to you because I’m feeling this paper is whispering to you… What do you all think?
Do Scrub Colors Affect Your Intelligence? A Study in JAMA Surgery Reveals Surprising Results
Elf Jonathan’s paper:
This is a study that explores whether what you wear affects how patients perceive you. It’s a heavy topic, but let’s talk about it in a tongue-in-cheek way. I don’t want to make light of the important literature around bias towards the visual representation of clinicians, so please take this in the spirit of what we’re talking about.
Hribar, C. A., Chandran, A., Piazza, M., & Quinsey, C. S. (2023). Association Between Patient Perception of Surgeons and Color of Scrub Attire. JAMA Surgery, 158(4), 421–423. https://doi.org/10.1001/jamasurg.2022.5837
The study was published in JAMA Surgery in May. It’s such an easy study to do, I wish I had thought of it! Here’s what they did: they asked 113 people who looked smarter and who looked like a surgeon based on the color of their scrubs. You might say, “Who cares? How does it match my shoes and all those other things?” But it turns out that the color of your scrubs matters more than you think.
So, what are the results? If you wear green scrubs, they think you look like a surgeon. If you wear black scrubs, they think you’re dumb and you don’t care. If you wear blue scrubs, they think you’re smart and kind. So choose your colors wisely, and let’s hope your patients don’t judge you by the color of your scrubs!
Elf Jason’s bonus article – Zooming Through First Impressions
Let me tell you about an extra paper that caught my eye. It’s all about how your zoom backgrounds can make or break your first impressions. This is very relevant for us, especially for John, who has a different style than the rest of us.
And guess what? The best background to have on zoom is…books! Yes, books! Now, Lara, what do you have in your background? And Linda, what about you?
Cook, A., Thompson, M., & Ross, P. (2023). Virtual first impressions: Zoom backgrounds affect judgements of trust and competence. PLOS ONE, 18(9), e0291444. https://doi.org/10.1371/journal.pone.0291444
And then, the worst background to have is something weird or quirky, novelty, like a stuffed animal or a lava lamp. John, what do you have behind you?
Holiday BINGO card!
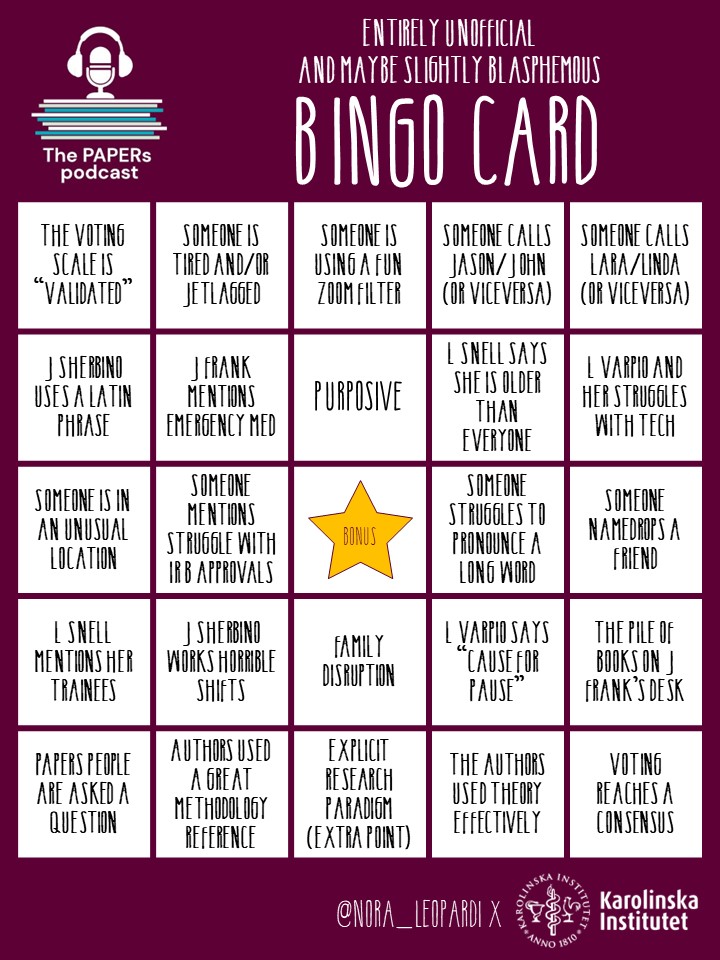
Play the PAPERs Bingo!
Challenge your colleagues and see who gets BINGO first. And try it on other episodes as well. What episode will you get most bingo on?
Creator

Dr Nora Leopardi @nora_leopardi (she/they) is a Lecturer in Clinical Education at the University of Newcastle, Australia. She is passionate about preparing current medical students to face the healthcare challenges that humanity will face in the next 50 years. Nora aims to foster self-regulated learning by creating effective, engaging and innovative teaching activities, which generate an authentic sense of curiosity and passion for learning in medical and health professions students. Nora’s primary fields of interest are learning environments, educational approaches and learning strategies, clinical reasoning, and Health Professions Education research. In her letter, Nora has asked Santa for IRB approval on that one project she’s been trying to run for a year.

0 comments