#66 – Assess or Stress? Factors Influencing Assessors in LMICs
Episode host: Jonathan Sherbino.

This episode dives into the rollercoaster ride of medical educators trying to grade students in diverse settings of the Global South, where intentions to assess are tangled up in personal quirks, self-confidence (or lack thereof), and the unpredictable chaos of their environment. Turns out, grading exams isn’t just about knowing the answers—it’s also about surviving a game of academic dodgeball with a healthy dose of “Can I really be bothered?”
Episode 66 transcript. Enjoy PapersPodcast as a versatile learning resource the way you prefer—read, translate, and explore!
Episode article
Sims, D. A., Lucio-Ramirez, C. A., & Cilliers, F. J. (2024). “Factors influencing clinician-educators’ assessment practice in varied Southern contexts: A health behaviour theory perspective”. Advances in Health Sciences Education.
Episode notes
Background
It’s time for my favorite topic – assessment. And with a second favourite running in parallel – challenging the assumptions of the global north. In this era of CBME (Competency Based Medical Education) a strong critique has been the operational cost/expense of programmatic assessment. Completing, collating, and confering a summary judgement requires both technological and human resource costs. In the Global North there has been legitimate concern about the ability to translate the theory of programmatic assessment into authentic practice. This challenge is magnified in low- and middle-income countries (LMICs).
Today we tackle the real-world challenge of the impact on learning and health systems when end-of-clerkship rotation summative examinations are designed and managed by a single individual.
Purpose
From the authors:
“Our research question was what factors influence the assessment practice of individual clerkship convenors in exit-level medical programmes in diverse Southern settings?”.
Sims et al. 2024
Methods
This is a qualitative study, adopting a constructivist paradigm with a model of health behaviour developed by the senior author serving as a theoretical lens. Health behaviour theories (HBTs) include the theory of planned behaviour, the transtheoretical model of change, social cognitive theory, self-determination theory, and more. Originally, HBTs describe the behaviours of individuals in relation to their health; in this context, it is transposed to assessors educational behaviours.
An eclectic model of Health Behaviour Theory
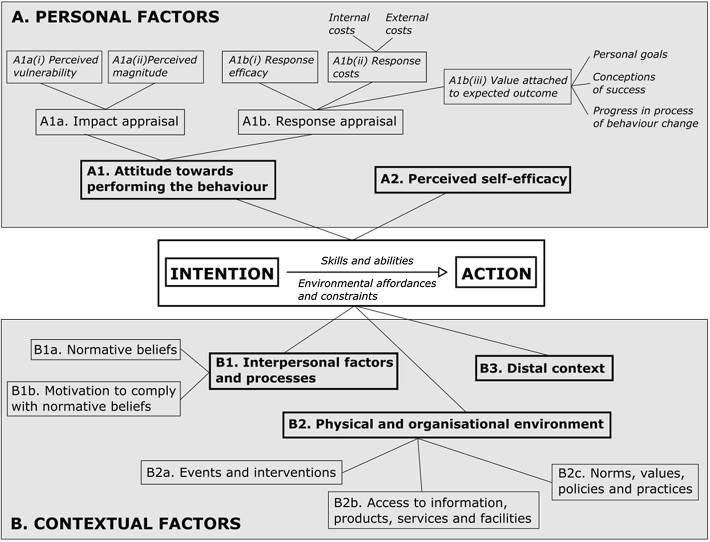
Put simply, the intention to perform an action is shaped by personal factors like attitudes and self-efficacy, as well as contextual influences such as interpersonal dynamics and environmental conditions. However, forming an intention does not guarantee action, as the move to action depends on an individual’s skills and the opportunities or constraints within their environment.
Semi-structured interviews (45 – 60 minutes), using convenience sampling of two public South African universities and one private, non-profit Mexico university, were conducted in the language of choice of the participant. Three questions were posed:
- How do you practice assessment in your clerkship?
- What personal factors influence your assessment practice?
- What contextual factors influence your assessment practice?”
(I think?) a generic thematic analysis was conducted. Of note, an independent review of the findings was conducted by the Mexican author, once the analysis was completed by the South African authors.
Results/Findings
Thirty-one clerkship convenors (i.e., clerkship rotation directors) were interviewed. Despite the convenience sampling strategy, there was diversity of gender, career stage, clinical discipline and social/cultural context.
In brief, an intention to act is informed by personal and contextual factors leading to action. If the intention is negative, as a function of impaired personal or contextual factors, then inaction results. The opposite is true if a positive intention is adopted by the assessor. The interplay of factors is complex and interdependent.
| Category | Factor | Influence on Assessment |
|---|---|---|
| Personal Factors | Attitudes | Influences behaviors positively or negatively; negative attitudes discourage assessment practice. |
| Impact/Consequence | Evaluates likelihood and magnitude of impact on self, students, and patients; negative appraisal discourages quality assessment. | |
| Opportunity Cost | Cessation of actions perceived as ineffective; negative impact if clinical/research work is prioritized over assessment. | |
| Self-efficacy | Low self-efficacy discourages assessment; reliance on more experienced colleagues. | |
| Contextual Factors | Interpersonal Factors | Strong leadership can inspire or enforce assessment change; resistance from unsupportive colleagues can deter intention. |
| Organizational Environment | Organizational resources and rules affects assessment practices; | |
| Assessment Training | Availability of training influences adoption of assessment practices. | |
| Assessment Expertise | Availability of expertise influences assessment design. | |
| Socio-cultural | Socio-political and historical contexts affect assessment practices; pressures may encourage or deter practices. |
Conclusions
“Personal competencies and conducive environments supported intention to action transition. While previous research has typically explored factors in isolation, the HBT framing enabled a systematic and coherent account of assessor behaviour. These findings add a particular contextual perspective to understanding assessment practice, yet also resonate with and extend existing work that predominantly emanates from high-income contexts in the global North. These findings provide a foundation for the planning of assessment change initiative…”
Sims et al. 2024
Paperclips
This manuscript is a good example of writing NOT hindered by an artificially mandated cap on word count. AHSE does not have a word count, nonetheless, authors must still consider parsimony and clarity in their writing.

0 comments